Next Step: Make Cards on the Automatic Key Concepts, and Vignettes
Remember, the more you automatically know what each sentence means on your test, the better you will do. There are 4 stages in making interpretation more automatic:
- Stage 1: Unable to Make Pathophysiologic Chronologies in Either Timed or Untimed setting
- Stage 2: Basic Pathophysiologic Chronologies, but with Significant Gaps
- Stage 3: Detailed Pathophysiologic Chronology Without Time, but Unable to Consistently Generate PC During Timed Setting
- Stage 4: Consistent Pathophysiologic Chronologies in Timed Setting
My goal with these vignettes is to help you reach Stage 4. How do you do so?
- With the Automatic Key Concept cards, you can master the underlying information to move past Stages 1 + 2.
- Then, with the Vignette/Pathophysiologic Chronology cards, you can teach yourself to make these connections on your exam.
Automatic Key Concepts:
Copy + paste these into your cards, to make these key concepts more automatic.
What is the mechanism of developing type 2 diabetes mellitus?
Insulin resistance → insulin overproduction → amylin production ↑ → amyloid production ↑ → βislet cell dysfunction → insulin demand >> supply → DM II
Walk through the baroreceptor reflex in response to a drop in blood pressure.
“Make a tattoo” MAP = CO x TPR = (HR x SV) x TPR; Preload, Afterload, Contractility
Baroreceptor stretch ↓ → sympathetic tone ↑ / parasympathetic tone ↓ →
β1 ↑ / M2 ↓ → phase 4 depolarization of SA node ↑ → HR ↑ → CO ↑ → MAP ↑
β1 ↑ → contractility ↑ → SV ↑ → CO ↑ → MAP ↑
α1 ↑ → afterload (TPR) ↑ → MAP ↑
How does β1 / M2 affect HR?
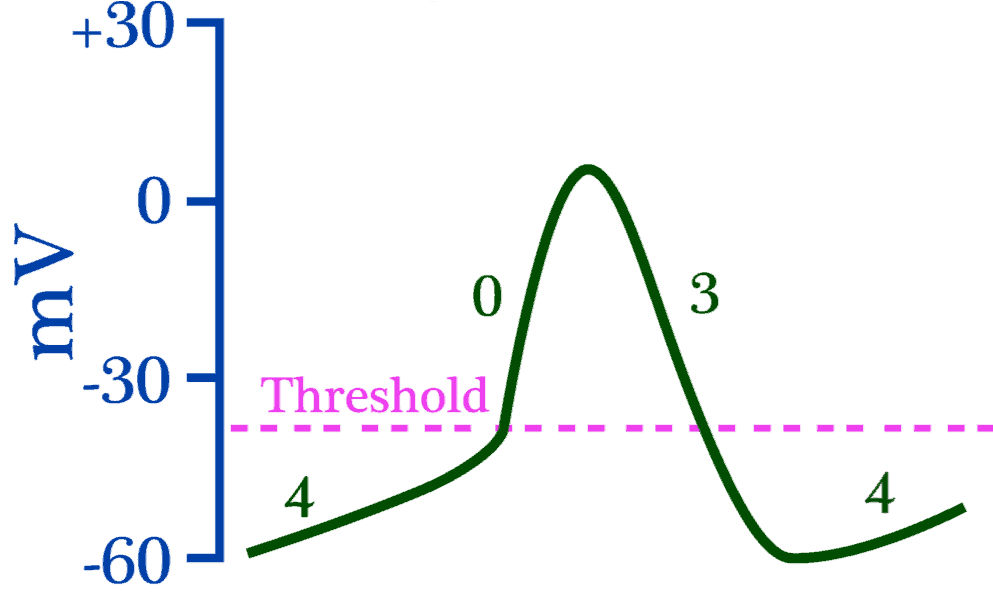
Change slope of phase 4 depolarization.
β1 → phase 4 slope ↑ → reach threshold faster.
M2 → phase 4 slope ↓ → reach threshold more slowly.
Someone presents with lightheadedness / syncope when standing. What is the general mechanism behind lightheadedness? Could this be a stroke?
Hypotension!!! Hypotension → CPP ↓ → brain hypoperfusion
Stroke is due to to FOCAL ischemia of the brain, and does NOT cause presyncope. Presyncope/syncope is almost universally hypotension.
What are the 3 elements in Virchow’s Triad?
Hypercoagulability, venous stasis, endothelial damage
If I had a pulmonary embolism to the right pulmonary artery, what would be the effect on the pulmonary arterial resistance? Think of the arteries as resistors.

PE to R pulmonary artery = like removing a resistor in parallel → total resistance ↑
In a PE, blood can’t flow through the artery that is blocked. It may seem odd to use the term “resistor” for a path that blood can flow through since colloquially “resistor” implies that it would somehow be harder to move through. That is not the case, however, for the use of “resistor” in this case – resistor simply means “conduit for blood.”
If it’s easier, you can think of it as, “a PE removes a conduit in parallel for blood to flow through → total resistance ↑”
Recall that resistors are in parallel if an electron could go through either one of them, but not both. Resistors are in series if an electron must go through both resistors to go from one point to another.
Blocking the distal branch of the radial artery would be removing a resistor in series, whereas blocking one of the many branches of the pulmonary artery would be removing a resistor in parallel. In the case of the branches of the pulmonary artery, blood could go through either the left or right pulmonary artery, but wouldn’t have to go through both.
How can a PE lead to hypotension?
Recall: MAP = CO x TPR.
PE → pulmonary artery blocked → pulmonary artery resistance (RV afterload) ↑ → pulmonary arterial flow ↓ → LV preload ↓ → SV ↓ → CO ↓ → MAP ↓
What is the mechanism of lower extremity edema in R heart failure?
Blood back-up into IVC → venous congestion, particularly in dependent areas of body → capillary hydrostatic pressure ↑ → fluid leakage into interstitium ↑ → pitting edema in lower extremities
Left vs. isolated right-sided heart failure: how can you differentiate between the two?
PULMONARY EDEMA!!!!
Left-sided heart failure → backup of blood into pulmonary capillaries → pulmonary edema → inspiratory crackles.
Signs of right-sided heart failure WITHOUT pulmonary edema (“lungs clear to auscultation”) = isolated right-sided heart failure
wow