![]()
Lessons Complete:
Next Step: Make Cards on the Automatic Key Concepts, and Vignettes
Remember, the more you automatically know what each sentence means on your test, the better you will do. There are 4 stages in making interpretation more automatic:
- Stage 1: Unable to Make Pathophysiologic Chronologies in Either Timed or Untimed setting
- Stage 2: Basic Pathophysiologic Chronologies, but with Significant Gaps
- Stage 3: Detailed Pathophysiologic Chronology Without Time, but Unable to Consistently Generate PC During Timed Setting
- Stage 4: Consistent Pathophysiologic Chronologies in Timed Setting
My goal with these vignettes is to help you reach Stage 4. How do you do so?
- With the Automatic Key Concept cards, you can master the underlying information to move past Stages 1 + 2.
- Then, with the Vignette/Pathophysiologic Chronology cards, you can teach yourself to make these connections on your exam.
Automatic Key Concepts:
Copy + paste these into your cards, to make these key concepts more automatic.
What is the mechanism of developing type 2 diabetes mellitus?
Insulin resistance → insulin overproduction → amylin production ↑ → amyloid production ↑ → βislet cell dysfunction → insulin demand >> supply → DM II
Walk through the baroreceptor reflex in response to a drop in blood pressure.
“Make a tattoo” MAP = CO x TPR = (HR x SV) x TPR; Preload, Afterload, Contractility
Baroreceptor stretch ↓ → sympathetic tone ↑ / parasympathetic tone ↓ →
β1 ↑ / M2 ↓ → phase 4 depolarization of SA node ↑ → HR ↑ → CO ↑ → MAP ↑
β1 ↑ → contractility ↑ → SV ↑ → CO ↑ → MAP ↑
α1 ↑ → afterload (TPR) ↑ → MAP ↑
How does β1 / M2 affect HR?
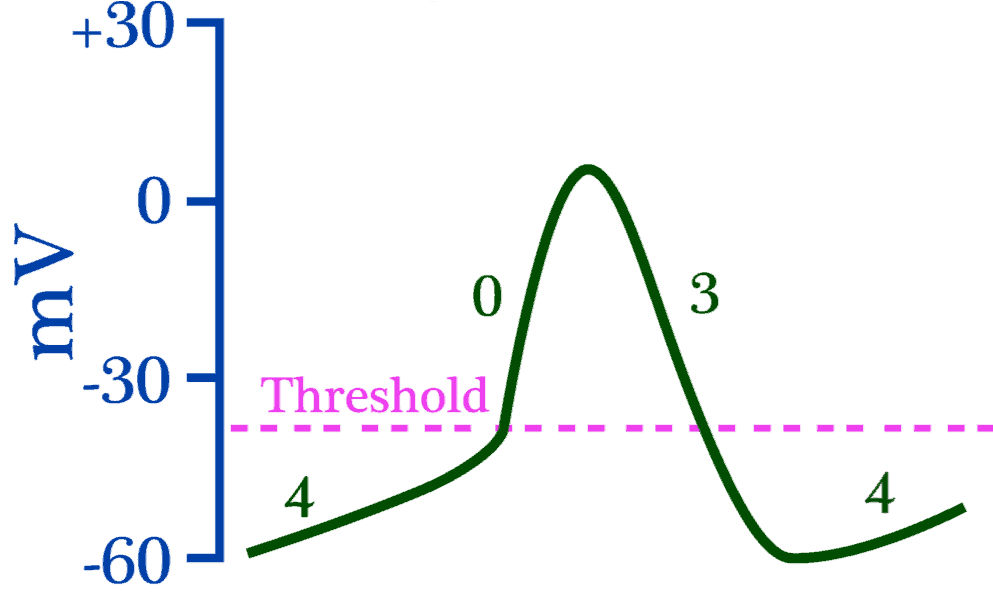
Change slope of phase 4 depolarization.
β1 → phase 4 slope ↑ → reach threshold faster.
M2 → phase 4 slope ↓ → reach threshold more slowly.
Someone presents with lightheadedness / syncope when standing. What is the general mechanism behind lightheadedness? Could this be a stroke?
Hypotension!!! Hypotension → CPP ↓ → brain hypoperfusion
Stroke is due to to FOCAL ischemia of the brain, and does NOT cause presyncope. Presyncope/syncope is almost universally hypotension.
What are the 3 elements in Virchow’s Triad?
Hypercoagulability, venous stasis, endothelial damage
If I had a pulmonary embolism to the right pulmonary artery, what would be the effect on the pulmonary arterial resistance? Think of the arteries as resistors.

PE to R pulmonary artery = like removing a resistor in parallel → total resistance ↑
In a PE, blood can’t flow through the artery that is blocked. It may seem odd to use the term “resistor” for a path that blood can flow through since colloquially “resistor” implies that it would somehow be harder to move through. That is not the case, however, for the use of “resistor” in this case – resistor simply means “conduit for blood.”
If it’s easier, you can think of it as, “a PE removes a conduit in parallel for blood to flow through → total resistance ↑”
Recall that resistors are in parallel if an electron could go through either one of them, but not both. Resistors are in series if an electron must go through both resistors to go from one point to another.
Blocking the distal branch of the radial artery would be removing a resistor in series, whereas blocking one of the many branches of the pulmonary artery would be removing a resistor in parallel. In the case of the branches of the pulmonary artery, blood could go through either the left or right pulmonary artery, but wouldn’t have to go through both.
How can a PE lead to hypotension?
Recall: MAP = CO x TPR.
PE → pulmonary artery blocked → pulmonary artery resistance (RV afterload) ↑ → pulmonary arterial flow ↓ → LV preload ↓ → SV ↓ → CO ↓ → MAP ↓
What is the mechanism of lower extremity edema in R heart failure?
Blood back-up into IVC → venous congestion, particularly in dependent areas of body → capillary hydrostatic pressure ↑ → fluid leakage into interstitium ↑ → pitting edema in lower extremities
Left vs. isolated right-sided heart failure: how can you differentiate between the two?
PULMONARY EDEMA!!!!
Left-sided heart failure → backup of blood into pulmonary capillaries → pulmonary edema → inspiratory crackles.
Signs of right-sided heart failure WITHOUT pulmonary edema (“lungs clear to auscultation”) = isolated right-sided heart failure
Vignette/Pathophysiologic Chronologies:
Copy + paste these into your cards, to make the connections behind these vignettes more automatic.
A 65-year-old man has poorly-controlled type 2 diabetes mellitus for 20+ years. He has progressive renal failure and tingling in his hands/feet. For the past several months, he gets lightheaded when he stands up from a seated position.
What is the pathophysiologic chronology?
Summary:
Heart failure and/or diabetic neuropathy of the autonomic nervous system → baroreceptor reflex dysfunction → (orthostatic) cerebral hypoperfusion
Detailed:
Born healthy, but poor lifestyle → insulin resistance ↑ → insulin production ↑ to compensate → amylin release ↑ → amyloid production in pancreatic β cells ↑ → β cell death → relative insulin deficiency → type 2 diabetes mellitus / blood sugar ↑ → non-enzymatic glycosylation of (peripheral) nerve axons → peripheral neuropathy (hand/foot tingling) + autonomic nerve dysfunction + kidney failure
Autonomic dysfunction → inability to compensate for preload drop when standing up (vagal nerve effect and/or decreased innervation of α1 receptors in blood vessels) → MAP ↓ → brain perfusion ↓ → pre-syncope (lightheadedness)
Alternative: DM2 → ischemic cardiomyopathy → ability to augment CO when standing ↓ → CPP ↓
A 67-year-old man comes to the emergency department because of a 1-week history of worsening left leg pain and a 2-day history of lightheadedness. He has a 1-month history of worsening upper mid-thoracic back pain, with 25-lb weight loss. His appetite has been unchanged. He has smoked 1 pack of cigarettes daily for the past 20 years. Heart rate is 100/min, and respiratory rate is 20/min. CT scan demonstrates a 2-cm mass in the pancreatic head, with an ultrasound of the left lower extremity demonstrating a femoral venous clot.
What is the pathophysiologic chronology?
Summary:
Smoking → pancreatic cancer
Smoking + pancreatic CA → DVT → PE → MAP ↓ → cerebral hypoperfusion
Detailed:
Born healthy → smoking → risk of pancreatic cancer ↑ → weight loss / retroperitoneal pain (pancreas = retroperitoneal organ → back pain)
Presyncope (lightheadedness): Virchow’s Triad 2 of 3: Pancreatic cancer (hypercoagulability) + smoking (endothelial damage) → (large) DVT → unilateral leg swelling/pain. DVT embolizes to lungs → blockage of pulmonary artery → LV preload ↓ → SV ↓ → CO ↓ → MAP ↓ → CPP ↓ → presyncope (lightheadedness)
Tachycardia: MAP ↓ → baroreceptor stretch ↓ → vagal nerve activity ↓ → M2 ↓ / β1 ↑ activity in SA node → phase 4 depolarization ↑ in SA node → HR ↑
A 36-year-old woman goes to the ED with complaints of sudden lightheadedness for the past 4 hours. She smokes and uses OCPs. She recently flew from Seoul to Los Angeles. Her jugular veins are distended, with lungs clear to auscultation. Her lower extremities have mild pitting edema.
What is the pathophysiologic chronology?
Summary:
Virchow’s Triad (3 of 3) → DVT → PE → right-sided heart failure / MAP ↓ → cerebral hypoperfusion
Detailed:
Born healthy → smoking + OCPs + venous stasis (Virchow’s Triad 3 of 3) → DVT → PE → pulmonary artery resistance ↑
Right-sided heart failure: pulmonary artery occlusion → back-up of blood into venous system → jugular venous distension/hepatomegaly/ pitting edema (capillary hypertension → fluid leaking into interstitium).
Clear lungs: no L-sided heart failure → no pulmonary edema → ”clear” lungs
Sudden presyncope: sudden PE → sudden drop in LV preload → SV ↓ → CO ↓ → MAP ↓ → CPP ↓ → presyncope (lightheadedness)
Links
FAQs
Audio Only
What is System 1 + System 2?
System 1 = your “intuition” or “gut” feeling
System 2 = critical/deep thinking
For a further discussion, see this:
When you talk about system 1 and system 2, what are you referring to?
System 1 = your “intuition” or “gut” feeling
System 2 = critical/deep thinking
For a further discussion, see this:
https://course.yousmle.com/courses/learning-strategy/knowing-the-right-answer-automatically
Thanks.
In Vignette #1, for the alternate pathophys for decreased CPP wouldn’t the baroreceptor reflex cause vasoconstriction to compensate and restore adequate CPP? Unless this mechanism be altered to begin with and we would still be left with the first chronology to explain lightheadedness anyway…. Is that correct?
Yes there is vasoconstriction, so the decreased in CPP will not be as much as it would be if there were no baroreceptor reflex. However, there is STILL a decrease in CPP, which would explain the lightheadedness.
Hi Dr. Palmerton,
Can you please explain why the pulmonary artery should be thought of as removing a resistor in parallel? Doesn’t click for me. Here is the flashcard from above:
“If I had a pulmonary embolism to the right pulmonary artery, what would be the effect on the pulmonary arterial resistance? Think of the arteries as resistors.
PE to R pulmonary artery = like removing a resistor in parallel → total resistance ↑”
Thanks!
Katie
In a PE, blood can’t flow through the artery that is blocked. It may seem odd to use the term “resistor” for a path that blood can flow through, but if it’s easier, you can think of it as, “a PE removes a conduit in parallel for blood to flow through”
Can you please explain the parallel part? Why can we think of it as in parallel?
See my response above – hope this helps!
Hi Alex,
Is this the correct understanding of the cause of vasovagal syncope?
urination/defication/ cough → preload ↑ → SV ↑ → CO ↑ → MAP ↑ → baroreceptor stretch ↑ → sympathetic tone decreases → β1 de-activation in the SA node → phase 4 depolarization slope slows → reflex bradycardia causing cardioinhibitory vasodepressor response
Thanks!
Interesting idea – honestly I don’t know what the cause of the increased parasympathetic tone is. Where did you come up with that mechanism? It sounds plausible! (Also, my name is Alec – I assume it was just a keyboard slip)
I was trying to figure out the pathophysiology of why vasovagal activates the vagus nerve → resulting in syncope. Do you have a better way to think of this?
I don’t unfortunately, sorry. Generally speaking, any sort of distress (hypoxia, hypoglycemia, etc.) leads to high autonomic tone generally – my guess is that it has something to do with parasympathetic tone somehow being higher than sympathetic tone, but that is purely speculative.
Hi Dr. Palmerton,
What’s the connection between Amylin and amyloid, is that the latter a byproduct of the former? I tried searching on the matter but simply got more confused. thank you.
Great question. I assume amylin was named that way because it was associated with amyloid – in other words, in people with high amylin (e.g., early DMII) they had accumulations of amyloid from the amylin. That is speculation, though. Amyloid, more generally, can come from LOTS of different proteins (presenilin in Alzheimer’s, amylin in DMII, etc.) – it is a superstructure of β pleated sheets, whereby overproduced proteins accumulate/aggregate together.
my Pc take for vignette #2 67 y,o male born healthy → risky health habits (smoking) for 20 years = injury to endothelium + 1 month upper back pain = 2 cm mass in pancreatic head. = hypercoagulability→ ⅔ virchow’s triad → risk of venous formation anywhere→ DVT → emboli to the lungs = PE → block in forward flow→ decrease preload in LA/LV→ decor SV = decor CO → decr MAP (MAP= CO x TPR) → low CPP (CPP = MAP – ICP) = low brain perfusion → syncope. PC on vignette #3 36 y.o female born healthy→ risky habits (smoking) =… Read more »
haha just listened to rest of the video, got it right. feels great Dr. Palmerton!
Great job! We provide “model” pathophysiologic chronologies so you can make your own, then compare them to what we have. Glad to see ours matched up!
How to organize the vignette in chronological order in time? we don’t have time to write down like this. We have to write in in our mind, right? how to train that?
Great question – yes, you do NOT have enough time to write them out by hand, but rather you will have to learn how to do this in your head. A lot of the speed will come from mastery of the concepts and knowing the major pathophysiologic chronologies in your head beforehand. You will NOT have enough time to construct new pathophysiologic chronologies for every vignette on your test. Rather, you need to know as many as possible beforehand, so you can simply “check” the vignette against the PCs in your head that you’ve already constructed. In this way, it… Read more »
how does β1 affect phase 4?
Increases the rate of depolarization → reaches threshold faster → HR ↑
Hi Dr. Palmerton, I had two questions from the Cardio anki cards: “Functional regurgitation = Incompetence of a valve stemming from an abnormality in one of its support structures (i.e. papillary muscles, chordae, and valve leaflets are normal).” – Shouldn’t the last word be ‘abnormal’ instead of normal?”In coronary artery disease, when give coronary vasodilators (e.g. adenosine and dipyridamole) → non-diseased coronary will dilate → blood flow through non-diseased coronary ↑ → blood flow through diseased coronary ↓. For a visual representation: https://qph.ec.quoracdn.net/main-qimg-f49160b41390eadb3a8bb22c20d98329-c” – the link did not open Why is preload increased in heart failure? Lastly, what is the… Read more »
No, it should be “normal” – that is the point. The valve is normal, but there is still regurgitation, hence “functional regurgitation.”
Heart failure = contractility ↓ → SV ↓ → amount of blood leftover after contraction ↑
Plus, heart failure → contractility ↓ → SV ↓ → CO ↓ → MAP ↓ → renal hypoperfusion → RAAS ↑ → Na+ reabsorption ↑ → volume expansion ↑ → preload ↑
Hi Dr. Palmerton,
One of the cardio anki questions mentions “In the ventricular myocytes, calcium channels contribute to the influx of calcium during phase 3 depolarization → ventricular contraction.”
However, I thought that phase 3 is due to K efflux from the cell (repolarization). I would appreciate it if you could clarify this. Thank you!
Thanks for the question, the card should say this:
“In the ventricular myocytes, calcium channels contribute to the influx of calcium during phase 2 depolarization (plateau phase) → ventricular contraction”
Thank you so much!
Dr. Palmerton, For the pathophysiologic chronology explained in the dashboard: “A 60-year-old man comes in with 4 hours of acute, left-sided chest pain. He has a past medical history of diabetes and hypertension. His temperature is 37 C, his HR is 95/min, and BP is 135/90. His EKG demonstrates ST-elevations in the inferior leads. The pathophysiologic chronology would be: DM + HTN (cardiac/vascular risk factors) → RCA plaque → rupture → RCA thrombus → posterior descending artery (PDA) flow ↓ → ischemia to inferior heart → left-sided chest pain / transmural infarction → ST-elevations in II, III, and aVF” My… Read more »
Yes, although honestly, I’m not sure how frequent is to have a PDA plaque rupture. But if it happened, then for sure it could cause an inferior MI.
Thank you!
You’re welcome!
Dr. Palmerton,
Why can’t hypoperfusion to the brain (↓ Cerebral perfusion pressure) cause a stroke?
Thanks!
It certainly can – prolonged brain hypoperfusion gives you watershed strokes, since the watershed areas are the ones that are least perfused, and thus most susceptible to ischemia. But remember the brain has an ischemic time of ~5 minutes before it causes necrosis (this is likely why status epilepticus is defined as seizures for 5 minutes or more, and why it is associated with necrosis – during a seizure the brain activity spikes → demand ↑↑ → demand > supply → ischemia → necrosis). So a short period of hypotension wouldn’t cause a stroke, but a prolonged one certainly could!
Wow, I never related this with status epilepticus. Thanks for the explanation!
You’re welcome!
Hi Dr. Palmerton,
For the Pathophysiology chronology for the first vignette (DM2 -> presyncope), would the damage to the autonomic nerves also include osmotic damage due to more glucose entering schwann cells -> aldose reductaase converts glucose to sorbitol -> osmotic damage ?
Yep – there are two major ways that hyperglycemia is thought to be bad for the body – osmotic damage (as you point out) and glycosylation of molecules (i.e., sugar starts adding itself randomly to proteins and other things in the body causing dysfunction in those things).
WOW! I’m just starting and this is my first actual lecture. Im in amazing awe! I can honestly say, while I knew the general principals, I would have missed sooooo many questions just because I had no idea of how to think chronologically…I can not explain how much of a difference this makes, but I am excited to answer questions from the Q bank today, just to see if I make a day one difference…WOW! thank you
That’s great!! So excited you’re able to start to see more of the pathophysiologic chronology behind each condition!
Hi Dr P
I couldn’t post comments until now .
I was giving it a try .
Hope you have a nice day 🙂
ok great! Glad it’s working now!
Hi! For the question about the man who smokes and has pancreatic cancer. How do you know he has a PE? I understand that Cancer leads to a hypercoagulable state which is why he had a DVT, but I don’t see any signs of lung involvement in the vignette.